When Your Doctor Is Full of Shit
When Your Doctor Is Full of Shit
Last month, The New Republic published an article titled “When Your Doctor Isn’t a Doctor” by Niran Al-Agba, a pediatrician in Washington state. To the extent that Al-Agba is known for anything, it’s for her one-woman crusade against nurse practitioners and physician assistants. The bulk of Al-Agba’s personal war is not waged in a clinical setting, but from behind a keyboard: Al-Agba is the co-author of Patients at Risk: The Rise of the Nurse Practitioner and Physician Assistant in Healthcare.
In a nutshell, Al-Agba’s professional focus seems to be less on patient care itself and more on ensuring that only the “right” people—i.e., physicians—be allowed to deliver it. If her ramblings were confined to the tens of tens of septuagenarians with paying subscriptions to The Kitsap Sun, it would be easy to ignore her. Alas, The New Republic chose to provide Al-Agba with a national platform, and the editors were apparently so awestruck by the “M.D.” after her name that they all promptly sank into their fainting couches and forgot to fact-check Al-Agba’s article before publishing it. Good thing I’m here.
[Full disclosure: My wife is a nurse practitioner (and, I’m willing to bet, a better clinician than Dr. Al-Agba. I’m not just saying that because she’s my wife; she’s really fucking good.)]
The piece begins with the story of Betty Wattenbarger, a seven-year-old autistic girl. I won’t recount all the details here, but in short, Betty had been sick for about four days. On the fourth day, her condition declined: her breathing was rapid, her lips were blue, she was lethargic and had no appetite, and her parents were rightfully concerned. Betty’s pediatrician was not seeing acute walk-in appointments that afternoon, and the pediatrician’s staff recommended that they take Betty to the nearest pediatric urgent care 30 miles away in Denton, Texas.
At Pediatric Urgent Care Denton, Betty was checked out by a clinician described by Al-Agba as “a woman with a stethoscope around her neck” who “did not introduce herself.” Eventually, the woman came back and informed Betty’s parents that Betty had tested positive for influenza A. Betty’s mother voiced her concerns about Betty’s rapid breathing, but the woman reassured her that Betty’s lungs were clear and that it was likely attributable to her high fever. Betty’s parents took Betty home.
The next morning, Betty’s condition had not improved. She fell in the shower; soon after, her father saw blood coming out of her mouth. Betty’s parents rushed her to the emergency room one mile away from their house, but it was too late. Betty had died.
After her death, Betty’s mother reviewed the medical examiner’s report and found that the M.E. had listed the cause of death as “sepsis complicating pneumonia with influenza A.” A deputy M.E. told the family that the influenza had made Betty susceptible to a bacterial infection (the pneumonia); the pneumonia spread to her bloodstream, and the sepsis occurred when Betty’s body released a flood of chemicals to fight the pneumonia. The M.E. also told the family that some of the cells in Betty’s left lung were already necrotic and there was “nearly half a cup of thick fluid” in her lungs, meaning it was likely that Betty had pneumonia when she was seen at the urgent care facility and it was overlooked.
Are you ready for the big twist now? Here it comes:
That’s how Al-Agba ends the story of Betty Wattenbarger: with a line break and a dramatic reveal that reads like it should be accompanied by an orchestral stab straight out of The Maltese Falcon.
A more responsible conclusion to draw from this would have been “This is an example of a clinician doing a bad job,” or maybe even “This is an example of a bad clinician, full stop.” Instead, Al-Agba uses the story of Betty Wattenbarger to make an entirely different point: “All nurse practitioners are hapless bozos masquerading as real doctors—and your child could be next.”
Once Ryan moved past his outrage, he noticed something strange about the article, something that a layperson might not pick up on:
Niran Al-Agba is full of shit.
It takes a lot of time and effort to become a physician. Most physicians put in this hard work because they want to help people, and what better way to do that than through the practice of medicine? But this isn’t always the case. Though they’ll never admit it, a lot of physicians aren’t all that passionate about helping people; it’s the status of being a physician that really soaks their socks.
Having a degree that tells everyone you’re the smartest person in the room? Oof buddy, that’s the good stuff. When someone calls you “Mister” and you get to interrupt and say “Uh, it’s Doctor, actually”? That’s what it’s all about right there. Starting every other story with “When I was doing my residency…”? Hook it to my fucking veins, brother.
You see this?

That’s an artist’s depiction of how these kinds of physicians feel when someone yells “IS THERE A DOCTOR IN THE HOUSE?” For them, medicine isn’t a calling. If they were ever passionate about medicine, that passion faded a long time ago. They get more satisfaction out of telling people that they’re a physician than they do out of actually being one. They look at patients the way someone working in a cubicle farm might look at rows of Excel data: as some tedious shit they have to take care of before they can clock out.
Did you know there are still message boards for physicians? And did you know that physicians spend a considerable amount of time on these message boards complaining that nurse practitioners are allowed to wear white coats? Here’s another example. And another. Here’s one of a physician complaining about an article about NPs, featuring a reply that says “DNP is a joke. I will never call a nurse a doctor.” In this one, a physician demands to know: “Why is a nurse practitioner prescribing me medication?” (Because they can, you absolute idiot.)
Of course, not every physician behaves like this. Most physicians respect NPs as clinicians and value the work they do. But there are plenty—like Dr. Al-Agba—who don’t and never will. And, as you’ll learn in a bit, it has nothing to do with patient safety or clinical outcomes. It’s just a turf war.
Betty Wattenbarger’s story was just the jumping-off point, and Al-Agba immediately turns to what she feels is the real issue here: that nurse practitioners are allowed to treat patients on their own. “[A]s many as 80 percent [of urgent care clinics] rely on nurse practitioners to oversee care, under what can only be assumed are varying levels of oversight by physicians.” Al-Agba briefly notes that “comprehensive studies on misdiagnoses and wrongful deaths at urgent care clinics are sparse”—which seems like the kind of information one should wait for before denigrating an entire profession as unqualified charlatans—before pivoting just as quickly to her next talking point: “what we do know is that nurse practitioners have as little as 3 percent of the clinical training hours undergone by physicians.”
The source she links to is an article on the National Institute of Health website titled “Should Nurse Practitioners Be Allowed To Practice Independently?” by Samer Cabbabe, M.D., President of the St. Louis Metropolitan Medical Society. (Oooh, sounds fancy!) A layperson might assume that since this was published on the NIH site, it must be accurate, but what most people don’t realize is that research is not automatically valid just because someone published it: you have to pay to get published, so journals are perfectly happy to run any old shit and let the reader determine for themselves if the study is worth a damn or not. But all too often, regular people who can’t tell the difference between a good study and a bunch of nonsense end up treating bad studies as gospel.
It’s less a study and more a shoddily researched op-ed, yet Al-Agba uses it as a foundational part of her argument against nurse practitioners. That can only mean one of two things: either she doesn’t know how to evaluate a study and just uncritically parrots anything that aligns with what she already believes (which speaks volumes about her skills as a clinician), or she knows it’s bullshit but thinks you’re too stupid to figure it out for yourself (which speaks volumes about who she is as a person).
Dr. Cabbabbabbe wastes no time in making it abundantly clear how he feels about nurse practitioners (emphasis mine throughout):
In order to become a nurse practitioner, students with a high school diploma usually study for a Registered Nurse (RN) certification, or for a degree in nursing. These degrees include the Associate Degree in Nursing (ADN) and the Bachelor of Science in Nursing (BSN) which can be completed in approximately two and four years, respectively.
That’s like saying “In order to become a physician, students with a high school diploma usually study for a degree in Biology.” It’s technically true, but it’s nowhere near accurate. (The actual requirements are outlined here; I wonder why Dr. Cabbabbabbabbabe didn’t think to use a legitimate source for this information? Hmm. Strange.)
He continues:
A new nurse practitioner, without any other nursing experience, acquires between 500 and 1,500 hours of clinical experience in a minimum of 1.5 years of postgraduate training, an equivalent of less than a third-year medical student. In contrast, a new family physician acquires more than 15,000 hours of clinical experience in a minimum of seven years post-graduate training.
This is where Al-Agba gets her “3%” figure from: 500 hours of clinical experience for NPs versus 15,000 hours for physicians. (Al-Agba also claims later in the piece that “nurse practitioners may be accepted into graduate school without having any prior nursing experience,” though she conveniently leaves out that 1) those programs are rare, and 2) a BSN in nursing is still part of those programs.) But the wording Dr. Cabbawitaba uses here is crucial: there is no such thing as “a new nurse practitioner without any other nursing experience.”
All nurse practitioners are RNs first. RNs are required to have at least 400 hours of clinical experience to sit for boards. In many states, you can’t practice as an RN without receiving a bachelor’s degree in nursing; in New York, RNs who received their license after December 10, 2017 have to obtain a baccalaureate degree in nursing within 10 years of earning their licensure, and BSN programs require anywhere from 700–1,000 clinical hours as part of the program. In other words, an RN could have anywhere from 700–1,400 hours of clinical experience before they even begin an NP program. (RNs who were licensed prior to the December 2017 cutoff are grandfathered in and don’t need to get a BSN if they don’t want to, but in order to start a graduate NP program you have to have a BSN.)
Even if a nurse practitioner only does the minimum 500 clinical hours required to sit for the national NP board exam, they would have at least 1,200 hours of clinical experience under their belts. At most, they’d have 3,900 total hours of clinical experience: 1,400 clinical hours as an RN, plus another 1,500 clinical hours as an NP. And at that point, they still have to maintain a written "collaborative practice agreement" with a physician for the first 3,600 hours of their careers. (Practice authority and scope of practice for nurse practitioners varies state-by-state.)
Add all that up, and by the time a nurse practitioner is allowed to practice independently in New York, they have anywhere from 4,800 to 7,500 hours of clinical experience—or anywhere from three to fifteen times as much experience as Dr. Crabapple claims.
Yeah, but that’s still a lot less than the 15,000 hours of training physicians get! Well, let’s take a look at that too.
Both Cabbabe and Al-Agba claim that a new MD has more than 15,000 hours of clinical experience and at least seven years of post-graduate training: four years of medical school plus a three-year residency. But the first two years of medical school are “pre-clinical” (meaning they don’t see patients), so they really have a five-year—not seven-year—window to accumulate 15,000 hours of clinical experience. That’s 3,000 hours a year, which means a third- or fourth-year med student is working 57.5 hours per week, 52 weeks a year, plus studying for their medical boards.
That seems pretty dubious to me, but the folks over on the message boards claim third- and fourth-year med students spend about 94 hours a week on clinical work. If that’s true (and it must be because they’re physicians), it begs the question: how can anyone actually learn anything—or retain what they’ve learned—when they’re working 16-hour shifts, 6 days a week? But I digress.
Sure, most physicians do a three-year residency because they get 1) extra training and 2) paid for it. Nurse practitioners don’t have that luxury. But physicians are not required to receive “a minimum of seven years post-graduate training”; a physician can sit for the state board exam after one year of a post-graduate internship if they want. That means that depending on their med school program, an MD could start practicing independently with as little as 5,760 hours of clinical experience.
A better way—certainly a more honest way—to compare the relative clinical experience between physicians and nurse practitioners would be to look at it from a different angle: what’s the least possible amount of clinical experience each group can have before they’re allowed to practice independently? In New York, that’s 4,800 hours for a nurse practitioner, compared to 5,760 hours for a physician. I’m no great shakes at math, but I’m pretty sure 4,800 is more than 3 percent of 5,760. Hang on, let me just…yep, it’s 83%.
Near the end of the piece, Al-Agba says that “nurse practitioners, physician assistants, and nurses are integral members of the health care team.” (This is, of course, immediately followed by her assertion that they should all work under a physician’s supervision.) Al-Agba’s halfhearted gesture towards evenhandedness is illuminating in its way: in her view, nurses, physician assistants and nurse practitioners are interchangeable cogs in the healthcare machine. In order to believe that nurses, physician assistants and nurse practitioners are in the same category, one would have to actively avoid learning anything about what nurse practitioners are trained to do. It’s a nice little sprinkling of insult atop a pile of injury: Al-Agba spends all her free time campaigning against nurse practitioners, and she hasn’t even bothered to learn the first thing about them.
So what’s the point of Al-Agba’s piece? Why go to such great lengths to denigrate an entire profession? Why does she deliberately and repeatedly cite misleading figures to make at seem as though the disparity in clinical experience between nurse practitioners and physicians is twenty-seven times greater than it actually is? Clearly she has an ax to grind about nurse practitioners, but where did that come from?
I can think of a few reasons.
Al-Agba’s contention is that she has nothing against nurse practitioners; it’s just about what’s best for the patient. But her attempts to position herself as a staunch and unyielding advocate for patient safety and patient health outcomes fall apart in the face of one key piece of information: the research does not support her argument.
A systematic review of 11 different studies (in other words, an actual study performed by actual researchers following actual academic and scientific guidelines) found that NPs “perform as well as physicians in terms of clinical safety and positive patient outcomes” and "matched or exceeded their physician counterparts in patient education and satisfaction.” At their best and allowed to practice to the limits of their license, a nurse practitioner can combine the clinical skill of a physician with the patient-first bedside manner of an RN.
This benefits everyone, including physicians like Al-Agba: allowing nurse practitioners to practice independently means physicians can spend less time reviewing and signing off on nurse practitioners’ work. It also reduces physician patient loads and allows physicians to provide better care to the patients they do see; that, in turn, improves the quality of care for patients and overall patient outcomes. And by allowing nurse practitioners to practice independently, patients have expanded access to good medical care.
(There are exceptions, of course: in some areas, patient outcomes and satisfaction are lower for nurse practitioners compared to physicians. Those areas also happen to be the ones in which nurse practitioners have limited or restricted practice authority. Like Texas, for example.)
So if it’s not about patient outcomes, what else could it be about? Well, there’s the financial aspect: if the secret gets out that a nurse practitioner can deliver the same clinical outcomes as a physician while improving on patient satisfaction, all for a fraction of the cost, there might be a lot less demand for physicians. It behooves physicians like Al-Agba to ensure that nobody else is allowed to do what they do.
But I don’t think that’s why. Nobody’s pushing to cut physicians’ salaries or replace MDs with NPs across the board, and if that were to ever happen (unlikely) it’d be long after Al-Agba is done practicing medicine. No, it’s not about money or protecting patient safety, or really even about patients at all. It’s about something much more simple and visceral: ego.
At its core, Al-Agba’s argument is about who should be allowed to wield the authority she currently enjoys; the only reason she even mentions patients at all is because they are the conduit for her authority as a physician. Only a certain kind of person is attracted to the field of medicine for the power and prestige, and they’re the same kind of person who finds it abhorrent that someone would infringe upon what they view as their territory—especially someone with the word “nurse” in their title.
Dr. Al-Agba might be a good clinician. She’s got good reviews, so maybe she's great at diagnosing patients and coming up with the right treatment plans to help them live healthy and happy lives. For her patients’ sake, I certainly hope so.
By my math, that makes her half as good a provider as my wife.
Despite never having Al-Agba in action, I’m 100% confident that my wife is every bit as good a clinician as Al-Agba, if not better. But while Al-Agba is busy Monday-morning quarterbacking the death of a seven-year-old to make false and wildly irresponsible claims about an entire group of medical professionals, my wife is busy busting her ass to make her patients’ lives better.
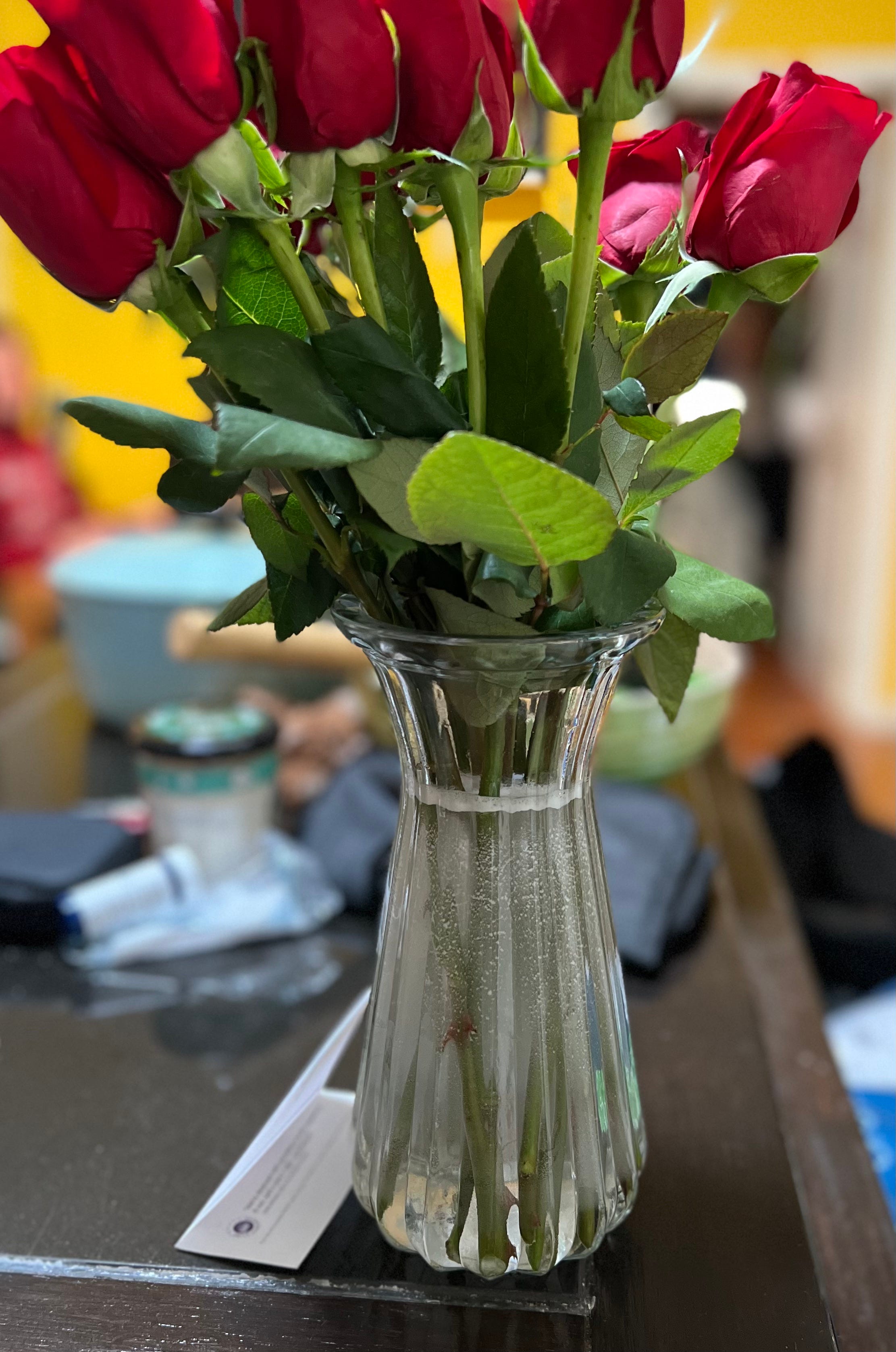
When’s the last time Al-Agba bought a shower chair with her own money so her patient who lost a leg to diabetes could safely take a shower in his new apartment—AND went there to help him set it up? When's the last time Al-Agba had a patient send flowers because they were so grateful that their provider actually listened to them? When's the last time Al-Agba's spouse delivered a brand-new wheelchair to one of her patients living in a homeless shelter because even though she was out of town sitting at her dying grandmother’s bedside, she still wanted to make sure her patients were taken care of? When's the last time Al-Agba butted heads with a parole officer so her terminally-ill patient could spend the last few days of his life with the handful of family members who hadn’t abandoned him? When's the last time Al-Agba cared enough about one of her patients to cry over them?
That’s the difference between my wife and someone like Al-Agba: my wife will absolutely hate that I’m bringing any of this up. She doesn’t do what she does for validation or praise. She doesn’t care about her title. When she calls Mount Sinai about one of her patients and some first-year resident asks her “who’s your attending physician?” she doesn’t write a book about The Rise of Dipshit First-Year Residents Who Don’t Know A Goddamn Thing. On the rare occasion my wife laments not going to medical school, it’s for one reason and one reason only: because it would make it easier for her to care for her patients without some message-board shitstain sneering that she’s just a nurse and refusing to listen to her (even though she’s right).
My wife is used to these kinds of people. I’m not. And it fills me with rage to know that while my wife is busy doing everything she can for every single patient she sees, someone like Al-Agba is out there making five times as much money to half-ass four patient visits a week. And when she’s not doing that, she’s busy telling anyone who will listen that she’s the good guy, and my wife is an impostor and a fraud who shouldn’t be allowed to help patients anymore. All in service of her fragile ego.
Fuck her.